
Exploring the Causes of Chronic Fatigue: A Collaborative Approach
“Health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.” WHO
Key Points:
- Fatigue is a syndrome that has many potential causes.
- An exploration into common measures in collaboration with a provider should be sought first unless certain concerns exist now or later in its development.
- Myalgic encephalomyelitis is a multifactorial neurologic condition that is associated with debilitation and exertional fatigue.
Table of Contents
- Preface
- Introduction: The Experience of Fatigue
- Chronic Fatigue: An Exploration into Causes
- An Approach to Investigating Fatigue
- Suggested Work-up of Chronic Fatigue
- Myalgic encephalomyelitis/Chronic Fatigue Syndrome: When to consider? What causes it?
- Further Reading and Resources
Preface
As an infectious diseases physician who searches for causes of an illness in patients when they are not always apparent, fatigue has been one of the most challenging conditions to address. Most of the time, additional testing will be required, if the cause isn’t detected from the beginning. I inform patients that I will continue to search on their behalf for a cause. I think to myself “is there one more test I can order, one more study that can shed light on their process.” Nevertheless, I am sometimes left without answers in spite of my attempts.
Some patients describe to me their experience from fully functional to being unable to work or keep other responsibilities. Initially, I considered a negative work-up an opportunity to work on other health issues that may be contributing: Do they have undiagnosed sleep apnea? Is obesity playing a role? Is there an adjustment reaction, prior history of trauma, or another sensitized state that is exacerbating it? These may be all be true, but I am often left with a feeling of an incomplete workup in a patient drastically looking for answers for their chronic fatigue. I have selected this topic for review, to raise awareness of this concern, and to carry on a dialogue of the journeys of readers who have had chronic fatigue.
My first experiences with fatigue did not occur as a doctor but as a patient. Within a period of 1 year when I was about 15, I had two viral conditions that gave me a chance to understand the difficulty that some people grapple with daily: measles and mononucleosis. These were strong motivators for me to become a doctor and an infectious diseases specialist.
While in Italy visiting relatives, we learned that my young cousin had just recovered from measles prior to our reunion. About 4 days after our first contact, I began with high fevers and body aches. Within a matter of days, the rash came and the spots in the mouth (I later learned in medical school that these were called Koplic spots). Along with these findings, I had extreme fatigue, where I couldn’t stand upright for longer than a few minutes. Over the course of a few weeks, the fatigue gradually lifted, and I eventually made it home.
Just about seven months later, I got mononucleosis from a girlfriend I was dating at the time (I later learned that people can spread mono for months after they had it. My throat became sore and swollen with white patches; lymph nodes in my neck swelled; a fever erupted. The fatigue peaked a few days later. I was confined to bed for the next three weeks, missing two weeks of school, and seldom leaving it but to take little steps to eat and use the bathroom.
Introduction: The Experience of Fatigue
The complaint of “tiredness” is common and reported in as many as 11% of 33% of patient visits. Although the majority of people who have recent fatigue have determinable health or psychiatric causes, a much smaller group struggles with chronic fatigue without any clear explanation determined.
The new designation for what formally was referred to as chronic fatigue syndrome is Systemic Exertion Intolerance Disease (SEID). Another term that may be more accurate is Myalgic Encephalo-myelitis; “myalgic” meaning muscle pain, “encephalo” meaning brain, and “myelitis” meaning inflammation of the spinal cord. The condition is characterized by a lack of energy that is not relieved with rest and is worsened with exercise. This can occur with impaired concentration, dizziness, and other symptoms. The process is debilitating for some, often leading to the need for bedrest after minimal exertion. Although women and individuals between ages 40 and 60 are most commonly affected, anyone can develop SEID/ME/CFS (I will refer to it as ME/CFS throughout the article).
Chronic fatigue is not an uncommon reason to seek consultation with a specialist, including in the field of infectious diseases. As a person explores possibilities with their physician, it is often challenging to develop an inclusive plan without bias or cognitive distortion. The workup often includes multiple referrals to specialists in the field of rheumatology, infectious diseases, hematology, and endocrinology.
Although infections can certainly cause fatigue, usually the investigation leads to more questions than answers. Even before a referral to a specialist, the primary care provider has already performed a battery of screening tests, including thyroid, anemia, and diabetes. A person can begin to fear that they may not ever have an answer; the condition may be exceptional or rare. This can motivate a patient to persist and seek further work-up or isolate themselves.
The sad truth is that medicine doesn’t always provide readily available answers for fatigue. There are multiple potential underlying causes that can lead to a similar presentation. There is yet to be a specific test that can identify the cause of fatigue. Rather than being one disease process, it might be more helpful to think of fatigue as a symptom – a manifestation of multiple separate and sometimes interacting causes. A battery of tests and treatment “Hail-Mary’s” may lead to further frustration. The best method to address fatigue starts with a thorough evaluation, active provider-patient dialogue, and a stepwise workup strategy.
There is yet to be a specific test that can identify the cause of chronic fatigue syndrome.
If the work-up is unrevealing, Myalgic Encephalomyelitis needs to be considered. A treat-while-evaluating pathway may be reasonable but isn’t always useful. At one point graded exercise and cognitive behavior therapy (CBT) was recommended for chronic fatigue syndrome, but have been shown to be ineffective and even contraindicated in this cause of chronic fatigue. Recently, the CDC removed its guidelines that included these measures for ME/CFS.
For physicians, understanding fatigue starts with providing a patient ample time for active listening and the acceptance of the words that they use to describe their experience. After months of debilitating fatigue, a patient may develop a narrative, considering some causes while dismissing others. A narrative does not necessarily entail that the person’s descriptions are inaccurate, just that they likely have told the story before. An attempt should be made to taking a non-biased, non-judgemental approach that considers possibilities to collaborate on the direction of further study. Anyone who has experienced chronic fatigue faces the fear of the unknown and the concern that their vitality might never return; a team approach and strategy are usually welcomed.
The article will address an approach to chronic fatigue, common modifiable causes of fatigue, and when to consider myalgic encephalomyelitis and its ramifications in this article.
Chronic Fatigue: An Exploration into Causes

The Parable of the 5 Blind Men and the elephant is a good metaphor to illustrate how important perspective is to evaluate problems like fatigue in the clinic. A different part of the elephant tells a different story. The trunk is like a branch; the tale is like a rope; the legs are like a tree stump. The elephant is all of these parts but much more.
When a person communicates an experience such as fatigue, they may use the words “fatigue,” “weakness,” “feeling drained,” or “tiredness,” but none of these words summarizes the same experience for every person. Words are subjective and require clarification. As we look for the source of one’s fatigue, the most important step in the process is listening to the narrative. Many times a good history may provide a potential cause of the fatigue or, in the least, a direction toward investigating it.
Questions to Consider with Fatigue
- Onset: Gradual or Abrupt
- Modify: Any behavior improves it? Does any behavior worsen it? Is the fatigue associated with increased activity?
- Associated Symptoms: Are there other symptoms that are noticed? Cough, shortness of breath, diarrhea, ulcers, easy bruising or bleeding, muscle pains, joint swelling, rash, heart palpitations, chest pain, abdominal pain, dizziness, thirst, weight loss, sleep problems, increased pain, etc.
- Medications: Do you take any medications to help you sleep (Benadryl, sleeping medications), to keep you awake (coffee, soda, stimulants), or to treat pain (opiates, marijuana, nonsteroidal).
Causes of Fatigue
Potentially serious causes of acute fatigue include blood loss, trauma, infection (acute endocarditis), or acute inflammatory or rheumatologic process, and they can usually be identified with a careful history, physical examination, bloodwork, and computed tomography (CT).
Aside from acute causes of fatigue, the causes of chronic fatigue can fall into several categories. It is important to remember that the body senses and responds to a disease completely, in both body and brain, such that the fatigue and stress state can interact and exacerbate one another.

Behavioral Factors in Chronic Fatigue
In some cases, does fatigue start in the brain? Studies have shown a significant association between fatigue and stress factors. To go back to the famous cartoon of a clinic visit, where a patient tells the doctor, “It hurts when I do this,” and the patient is banging his head with a pan, or there is an arrow in the patient’s backside. Bottom line: there are things that we do each day, whether we realize it or not, that can lead to fatigue. In individuals with ME/CFS, these behaviors can exacerbate the process.
-
- Sleep. Approximately one-third of US respondents related that they slept less than 7 hours a night (a study from the CDC which evaluated the 2014 Behavioral Risk Factor Surveillance System n=444,306). Sleep deprivation (see a previous YHF article here) is associated with multiple health concerns, including cognitive dysfunction, high blood pressure, increased stress. If you are trying to get enough rest, but are finding yourself waking up frequently at night, you might benefit from sleep apnea screening. If you are unable to fall asleep, consider revisiting sleep hygiene measures and limited coffee, soda, and other stimulants in the afternoon. If you find yourself drinking more than two cups of coffee a day or caffeinated soda, you might be self-treating the fatigue of sleep-disordered breathing.
- Fibromyalgia and ME/CFS have many overlapping features, and sleep deficit or sleep-disordered breathing has been shown to exacerbate both of the conditions. Here is a link to detail the differences and similarities.
- One study compared performance scores after increased wakefulness to that of alcohol intoxication: psychomotor impairment (risk for accidents, etc) after increased wakefulness corresponded to higher blood alcohol levels, so that after staying awake for 24 hours was equivalent to a blood alcohol level of 0.10% (above the legal limit for driving)!
- Substance Use. Alcohol is a depressant and can be associated with sleep impairment, inflammation, and fatigue. If you are drinking alcohol regularly, it may be affecting your energy level. Otherwise, it does exacerbate chronic fatigue. Studies on ME/CFS have shown that people with the condition curb or stop regular use of alcohol, reporting alcohol intolerance.
- Stress Level: There has been an association found with people who report chronic fatigue and level of stress. Dobbins et al found that 95% of patients with ME/CFS reported a stressful event at onset (Dobbins JG, 1995). Stress has been found to decrease the ability of the immune system to contain infections. The sympathetic nervous system is a reaction to stress, leading to a rise in serum cortisol and heart rate and triggers inflammatory markers. (See causes of ME/CFS).
- Trauma: Trauma is a very important risk factor and is associated with chronic fatigue syndrome. There was a six-fold higher association with childhood trauma in study subjects with CFS compared with controls (Heim, 2009).

Work-up of Chronic Fatigue
Chronic fatigue requires a multi-disciplinary approach. The following topics are meant to be a guide in the evaluation of fatigue in the outpatient setting and are not intended to be comprehensive or replace consultation with a physician or other provider and a detailed intake and examination. I am aware that some of these details may be outside the scope of the general reader, and I have tried to define the terms within the sentences.
- History/Physical examination:
- In the intake of the patients history, I listen closely for conditions that may overlap with chronic fatigue syndrome and fibromyalgia, including migraines and irritable bowel syndrome. I ask them of any family history of fatigue (possible genetic link in some), and any personal history of any traumatic childhood experience (Adverse Childhood Experiences (ACEs), which have been closely tied to the development of chronic diseases, including fatigue syndromes, as adults. I ask them if they have had any history of major anxiety or depression), since these may overlap with fatigue. I carefully review any medications and any substances that they are taking, since some medications may have untoward side effects including fatigue (beta-blockers, diuretics, antihistamines, some anti-depressants).
- Skin and nail examination: I perform a detailed skin and nail examination. Generalized infections and other conditions (sarcoidosis, squamous cell carcinoma, Kaposi’s sarcoma, inflammatory bowel disease) can have findings on the skin. I often consider a biopsy if there is a concern of this. Nail bed changes can be seen with subacute infectious endocarditis, diabetes, chronic liver, and kidney conditions.
- Blood pressure: can be low in adrenal insufficiency, atrial fibrillation. can be high in hypothyroidism, hyperthyroidism, hypercortisolism, or sleep apnea
- Pulse rate: tachycardia (fast heart rate) is a common cause of fatigue given impaired reserves. It can be seen with hyperthyroidism, atrial fibrillation, use of stimulants (meth), Postural orthostatic tachycardia syndrome (POTS). A slow heartbeat can cause fatigue as well; it can be seen in various forms of heart block, Lyme disease (Lyme carditis).
- Orthostatic vital signs: This is a test to check for a drop in blood pressure and an increase in pulse past the usual time of adjustment with a change in position. The drop can be seen with autonomic dysfunction (a condition seen in diabetes and Parkinsonism), adrenal insufficiency (when not enough cortisol is secreted). This is an important exam that is often omitted in most clinic visits. l check lying, sitting and standing with at least 3-minute intervals for both pulse and blood pressure. A blood pressure drop of greater than 20 mm Hg or a pulse rate greater than 15 is a positive test.
- Other/Exam: A pulse oximetry showing low oxygen levels can certainly give a clue that the process involves the oxygenation of blood (shunt, certain infections, (PJP/Covid-19) chronic pulmonary thrombosis). An exam of the heart identifying a murmur may raise the concern for a valve abnormality causing fatigue, including aortic stenosis, endocarditis, and mitral regurgitation. Check for enlarged organs such as the spleen or liver, which can be a sign of cirrhosis, hemolytic anemia, hemochromatosis, etc.
- Bloodwork: The following are reasonable considerations in evaluating someone with fatigue when the history and physical do not completely point to a cause. I would mention that it may be reasonable to start with basic screening or tailor it toward the presentation.
- CBC with Diff for anemia (low red blood cell count, low hematocrit from iron deficiency anemia and/or chronic blood loss), elevated hematocrit (can be seen in sleep apnea or polycythemia), platelet count (elevations can be seen in inflammatory conditions; low levels can be seen in cirrhosis or other platelet disorders ITP/TTP.. Check Iron studies if anemia or microcytosis (also consider thalassemia in some)
- Comprehensive metabolic panel for liver function tests a marker of liver disease and inflammation; kidney functions (creatinine and blood urea nitrogen) for evidence of kidney dysfunction and buildup of nitrogen products in kidney disease. Low sodium and low/high potassium or other electrolytes. Low sodium can be seen in Syndrome of Inappropriate ADH secretion (SIADH; precipitated by an underlying condition or medication). High potassium levels (and low glucose levels) may be seen with adrenal insufficiency. Low potassium could be seen in a potassium-wasting condition like Bartter’s or Gitelman’s syndromes or from abuse of diuretics or laxatives). Diabetes can sometimes present with fatigue as well. There is an association between cirrhosis and other liver disease and fatigue.
- Thyroid-stimulating hormone (TSH). This is the screening test for thyroid dysfunction. There is no need for T4/T3, Free T4/Free T3. If there are any concerns for autoimmune conditions (“swelling in the neck” to suggest thyroiditis) then check thyroglobulin Ab, and tissue peroxidase antibody (TPO) for Hashimoto’s thyroiditis which can be associated with other autoimmune conditions.
- Vitamin D levels (1,25 hydroxyvitamin D) – this is the correct form to check for insufficiency and deficiency. There has been some correlation between fatigue and low vitamin D levels, with improvement after replacement (Roy et al, 2014).
- Erythrocyte Sedimentation Rate, C-Reactive Protein. These are tests which show inflammation can signal ongoing smoldering. An elevated ESR or CRP may be seen in a rheumatologic process, such as rheumatoid arthritis (along with the history), polymyositis, or temporal arteritis, and infections such as endocarditis, relapsing fever, Lyme disease, etc.
- Other tests: Depending on the history, I may order triglycerides (associated with an inflammatory diet), uric acid (gout), calcium (hypercalcemia can be associated with fatigue), a stool for fecal elastase if I am concerned about malabsorption syndrome from chronic pancreatic dysfunction (exocrine deficiency), blood cultures (for endocarditis), peripheral blood smears (to look for unusual cell lines), HIV testing, Hepatitis B testing (Surface Ag and Ab), Hepatitis C Antibody testing. EBV and CMV tests require consideration, but I usually do not order these. They can be challenging to interpret, because they are usually serologies (and remain positive after prior infection); 90% and 80% of adults have these conditions, respectively. Studies looking for active replication of EBV, CMV and HHV-6 have not found a consistent association with Chronic Fatigue Syndrome compared to controls. In HIV, we will occasionally see reactivation of EBV and CMV and associated conditions of colon and central nervous system (brain) lymphoma (EBV) and retinitis and esophagitis (CMV).
Additional testing/next steps:
Depending on the results of the above, further testing may be needed in the direction of the history, physical examination, and lab findings. The following are options:
- Cosyntropin (ACTH) stimulation test. I use the 0.25mg dose and check AM cortisol and ACTH levels before the test and levels one hour following the dose. People who are on long-term steroid therapy (usually greater than 5-10mg) and chronic pain medications may develop adrenal insufficiency and experience fatigue. Anyone who has a positive orthostatic hypotension test also gets a follow-up stimulation test to look for adrenal insuffiency.
- Chest radiograph (PA/Lateral): Tuberculosis, Mycobacterium avium-intracellulare and other lung infections can present with fatigue (and usually some form of lung symptom like cough and shortness of breath). A lateral might be useful to look for hilar (the central area of the lungs where the largest branches) lymph nodes.
- ECG and 2D-Echocardiogram: This is a useful test in screening patients who have fatigue, along with shortness of breath and/or chest pain. It isn’t uncommon that a person has significant fatigue following a heart attack (sometimes for several months or longer). One study found 50% of subjects had significant fatigue following a known myocardial infarction. Sometimes a person may have fatigue when they have chronic heart disease, including ongoing ischemia (when the blood supply is diminished in the heart), a prior silent heart attack (more common in elderly and diabetics),valve issues, and atrial fibrillation. I once diagnosed a patient with atrial fibrillation who was convinced he had a chronic tick-borne infection after a trip to China, when I noticed that he had a very irregular pulse.
- Other radiologic: CT scan Abdomen/Pelvis (when iron deficiency anemia, weight loss, elevated liver tests, and/or abdominal pain); MRI of the brain if any concerning findings of headaches, visual symptoms, and new-onset seizures. MRI changes have been found in ME/CSF.
- Sleep study: This should be considered in anyone with non-restorative sleep, secondary insomnia (waking up at night), or nighttime urination (nocturia). Eighteen million Americans have obstructive sleep apnea (OSA); The majority do not know they do; some learn of the condition when they develop a complication from it. Anyone with undiagnosed chronic fatigue should consider a screening sleep study as part of the work-up.
- Serologies and other: There are no clear strategies to testing serologies. This article will not go into detail on Lyme testing and treatment. However, Lyme serologies with confirmatory Western Blot may be appropriate to consider, though there are no clear protocols for when to test. Most patients that I see in the clinic with “chronic fatigue” usually have been tested for it. Chronic infection has been shown (persistent skin findings) as well as a post-treatment Lyme disease syndrome (PTLDS), which is not believed to be caused by lingering infection. Here is a current article from BMJ on Lyme disease. Other tests include serologies for Coxiella burnettii, Trophyrem whipllei, and Borrelia recurrentis, and the Quantiferon IGRA.

Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
An individual who has experienced significant fatigue in lieu of any obvious abnormalities in bloodwork or other studies may have myalgic encephalomyelitis. The most common symptoms is post-exertional fatigue or malaise (PEM). As many as 48% with ME/CFS are incapable of engaging in productive activity; the majority (59%) describe a fluctuating course (Chu et al, 2019). The CDC estimates that 836,000 to 2.5 million Americans suffer from ME/CFS. Refer to the CDC Website for more information.
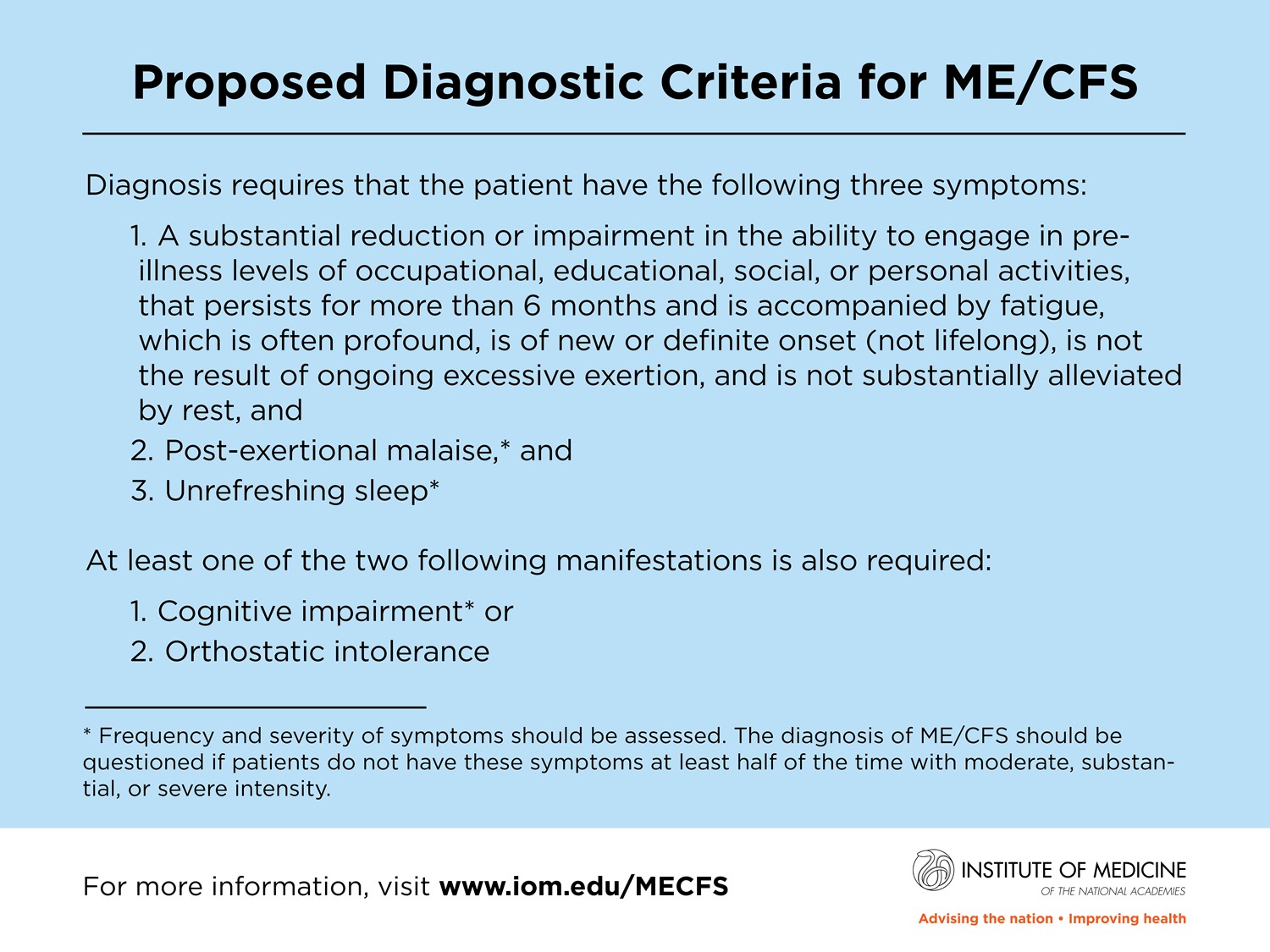
Diagnostic Criteria of ME/CFS/SEID
The criteria for diagnosis are as follows (Reference) :
- Reduction or impairment in the ability to engage in pre-illness levels of activity.
- Duration greater than 6 months
- Fatigue is often profound, new, not tied to excessive exertion, not substantially relieved by rest or sleep.
- Post-exertional malaise (PEM). Relapse can occur after exertion may last days to weeks.
- Unrefreshing sleep – non-restorative sleep without other underlying explanation.
Additional (one of the two other findings):
- Cognitive impairment, trouble with thinking and/or psychomotor impairment; trouble keeping normal schedules.
- Orthostatic intolerance, symptoms become worse when standing
Possible Causes of ME/CFS/SEID
Although ME/CFS has multiple potential associations, the most common processes reported with the syndrome were infection-related (64%), a stressful incident (39%), and exposure to environmental toxins (20%) (Chu et al, 2019). It is difficult to completely determine the causes on the basis of reporting; an association with dysregulation after certain viral infections, including HSV, EBV, CMV has been found; further studies to determine the potential causes and pathophysiology of ME/CFS are needed.
A more recent concept that approaches the multi-systemic interactions in the body is known as the psycho-neuro-endocrine-immune system (PNEI). Within the vascular system, the body responds to the intake of various injuries, toxins, allergens, and pathogens by unleashing myriad cell signals, including cytokines and interleukins, and cells to the site. These result in inflammation that induces inflammation and enables healing. This is likely the putative process in conditions such as atherosclerosis, multiple sclerosis, inflammatory bowel disease, cancer, and autoimmune conditions.
Microbes, such as viruses and bacteria, have been associated with ME/CFS. These include Enteroviruses, Epstein-Barr virus (EBV), Cytomegalovirus (CMV), Human Herpes virus-6 (HHV-6), Parvovirus B19, Hepatitis C, Chlamydia pneumoniae, Coxiella burnetii.
COVID-19 and Chronic Fatigue.
The Morbidity and Mortality Weekly Report (MMWR) published an article in July describing a delay in return to the usual state of health of 35% of patients interviewed between 2 and 3 weeks after the test date and after hospitalization. Prolonged symptoms included cough, fatigue, or shortness of breath, and was more common in people greater than 50 years of age (47% compared to 32% ages 35-49). A multi-year collaborative study is underway to determine the extent to which COVID-19 may lead to the development of ME/CSF.
ME/CFS and Inflammation
To determine if there were inflammatory markers found in those with ME/CFS, 192 subjects with the condition were assessed for serum cytokine compared to 392 healthy controls in one 2017 study. There were levels of TGF-Beta that were elevated and among 17 cytokines, there was a statistical upward trend in those with ME/CFS compared to controls. Thirteen of these cytokines are known to be pro-inflammatory.
The Stanford ME/CFS initiative showed in a retrospective review that fifteen patients with this condition had MRI’s findings of bilateral white matter atrophy compared to controls. A distinctive feature of degeneration of crossing nerve fibers was also noted in the right arcuate fasciculus in these patients. (Zeineh et al, 2013). Other radiologic studies using PET scans have also shown neuroinflammation in patients with ME/CFS, those with worse disease showing more inflammation, suggesting that inflammation plays a role in the process (Nakatomi et al, 2014). Additionally, a widespread reduction in the serotonin 1A receptor binding potential was found, particularly in the hippocampus and anterior cingulate (Shan et al, 2020).
It is conceivable that the triggering process, whatever it may be, leads to an autoimmune response, beginning with damage-associated molecular proteins (DAMPs) in the vascular system which triggers a similar cascade in the brain. ME/CSF has similarities with conditions such as Multiple sclerosis. Whether viral reactivation from e.g. Epstein-Barr viruses in tissues in a setting of ongoing stress (leading to cortisol release and weakening cellular immunity) further fuels this reaction is still unclear. EBV activation has been the source of various cancers including nasopharyngeal carcinoma, post-transplant lymphoproliferative disorders (PTLD), and Burkitt’s lymphoma (Kerr J, 2019).
Patients with ME/CFS have also been found to have increased expression of EBV induced gene 2 (EB12), found in the setting of EBV reactivation (Kerr J, 2019). Although some correlation is present, EBV reactivation as a trigger in some people with ME/CFS is still a hypothesis and requires ongoing studies to confirm; likely the same can be said for CMV and HSV, other Herpes viruses that are regulated by the immune system but are known to reactivate in some conditions.
A novel biomarker blood test for ME/CFS?
This month (Nov 2020) an article was published looking at possible bloodtest for ME/CFS (Nepotchatykh, 2020). The researchers looked at eleven microRNA expression (miRNA) before and after a post-exertional malaise (PEM) simulation, using a therapeutic massage device. These MicroRNAs are associated with immune regulation and inflammation. Although more validation is needed, these studies may pave a pathway for a new test for ME/CFS.
Fatigue Treatments
This will be subject of part two.
Fatigue Worksheets
Below is the Fatigue Severity Scale. Each of the questions is answered with a point value from 1 for “Strongly Disagree” to 7 for “Strongly Agree.” The maximum score is 63 points; the higher the score is, the greater the experience fatigue.

Summary
The article covers the complex issue of fatigue, presenting important risk factors and causes specific to chronic fatigue. A collaborative approach between provider and patient can be helpful in problem-solving the direction of the work-up and identifying important causes of the fatigue. The entity known as Myalgic encephalomyelitis can be a debilitating inflammatory process, usually with a fluctuating course. It is with hopes that exploring risk factors and associated conditions may provide support to address all causes of fatigue in a multi-faceted effort.
Questions for the Reader
Have you had any personal experience with fatigue? How did you address it? How did it get better or more manageable?
Bibliography
Chu L, Valencia IJ, Garvert DW, Montoya JG. Onset Patterns and Course of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Frontiers in Pediatrics. Feb 2019 Vol 7 (12): 18-35
Dobbins JG, Natelson B, Brassloff I, Drastal S, Sisto S-A. Physical, behavioral and psychological risk factors for chronic fatigue syndrome: a central role for stress? J Chronic Fatigue Syndr. (1995) 1:43-58.
Heim C et al. Childhood trauma and risk for chronic fatigue syndrome: association with neuroendocrine dysfunction. Arch Gen Psychiatry. 2009. 66(1):72-80.
Kerr J, Epstein-Barr virus Induced Gene-2 Upregulation Identifies a Particular Subtype of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. Frontiers in Pediatrics. 13 Mar 2019. Vol 7(59):47-57.
Nakatomi Y, et al. Neuroinflammation in Patients with Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: An 11C-(r)-PK11195 PET Study. J Nucl Med. June 1, 2014 vol 55 (6):945-950.
Nepotchatykh E, et al. Profile of circulating microRNAs in myalgi encephalomyelitis and their relation to symptom severity, and disease pathophysiology. Scientific Reports. Nov 2020. 10:19620
Roy S, Sherman A, Monari-Sparks MJ, Schweiker O, Hunter K. Correction of Low Vitamin D Improves Fatigue: Effect of Correction of Low Vitamin D in Fatigue Study (EViDiF Study). N Am J Med Sci. 2014 Aug; 6(8):396-402.
Shan Z, et al. Neuroimaging characteristics of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): A Systemic Review. J Translational Med. 2020. 18, 335.
Zeineh M, Kang J, Scott A, Raman M, Reiss A, Norris J, Valencia I, Montoya J. 2014. Right Arcuate Fasciculus Abnormality in Chronic Fatigue Syndrome. Radiology. Vol 274(2)
Further Reading
Advances in ME/CFS Research and Clinical Care. Frontiers in Pediatrics and Frontiers in Neurology. Edited by Friedman K, Bateman L, Bested A, and Nahle Z. Nov 2019.




{kind=link}
Leave a Reply