59 year old with Meningitis, Lung Cancer, Confusion, and Brain Lesions
Written by Charis Bush, OMS IV, edited by Christopher Cirino, DO MPH
Case Report: A 59-year-old male presents with 7 months of headache and nausea, along with 30 lbs weight loss
in that time period. He was found to have an abnormal screening chest x-ray which demonstrated a lung mass in the left lower lobe concerning for malignancy. He underwent a CT and CT-guided biopsy that arrived at the diagnosis of adenocarcinoma.


During the development of his symptoms, he also reported intractable nausea, vomiting, and dizziness refractory to medications. As part of his evaluation with the oncologist, he received a CT scan of his brain and a follow-up MRI ordered by a neurologist. The radiologist raised some concerns about a potential infectious process causing encephalomeningitis. The oncologist arranged for the patient to have a lumbar puncture to rule out infectious disease.
After the oncologist was called for concerning findings on the lumbar puncture, she referred the patient to the emergency department to be admitted.
EMERGENCY DEPARTMENT:
The patient describes bouts of nausea and vomiting for over 7 months. There has been a bitemporal headache almost every day for about the same length of time. He reported vision changes which he attributed to getting older but denied new blurry vision or other visual disturbances. The patient did notice some cognitive decline in the last 6 months. He reported some hallucinations as well in the days preceding the admission.
He noticed weight loss over the last several months as well.
He denies acute weakness, numbness, or tingling. He denies fevers,
chills, chest pain, shortness of breath, diarrhea, or dysuria; no recent travel or sick contacts. He has a female partner. He denies any history of STIs. He quit smoking 1ppd and use of heavy alcohol as things were developing and when he was diagnosed with cancer.
Physical exam in ED:
Vitals: Temp: 98.4, HR:78, RR:16, BP: 122/93, SpO2: 96% RA, weight 71 kg
The physical exam including a comprehensive neurological exam was unremarkable and non-focal.
Looking back —
Two months prior to his ER presentation, his MRI revealed:



MRI result: Bilateral lesions in the basal ganglia left greater than right predominantly in the putamen. These are
high signal on T2, low signal T1, prominent on FLAIR and demonstrate enhancement following
gadolinium. These are new compared to the previous examination in August. Differential
considerations include infection such as cryptococcal meningitis. (However, no leptomeningeal
enhancement) Acute disseminated encephalomyelitis or drug reaction are considerations.
ADMISSION:
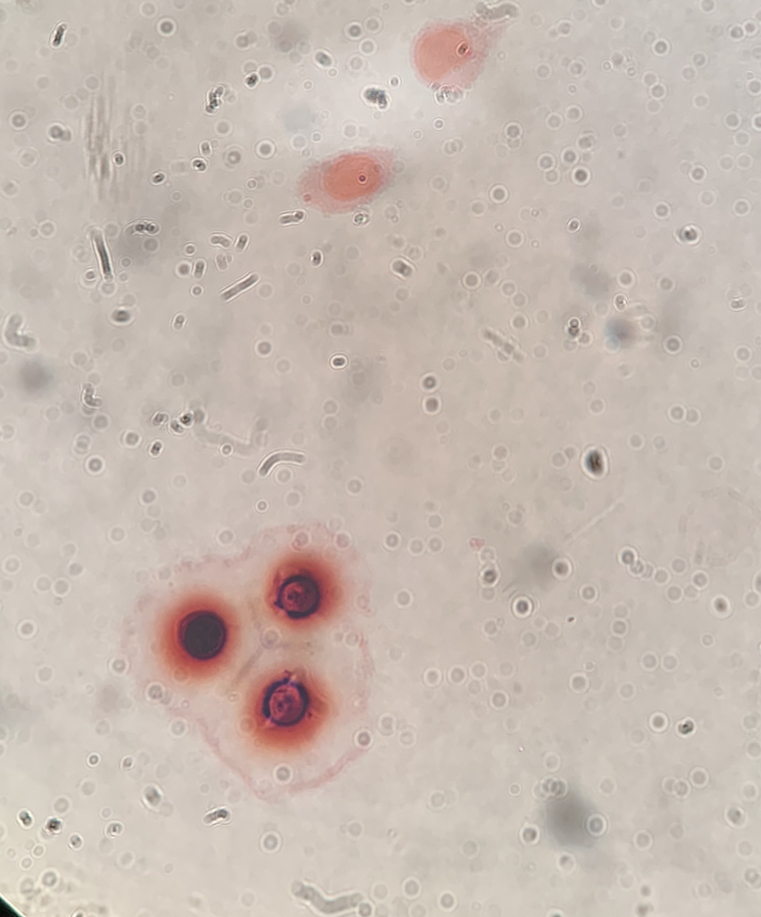
The patient was admitted to the hospital after a lumbar puncture result showed yeast in the CSF (pictured below). He had primary lung adenocarcinoma with no
obvious or significant risk factors or immunosuppression for a fungal meningitis other than his current cancer diagnosis.
The Repeat Brain MRI on admission:
Axial views: Nodular enhancements amongst bilateral edematous brain parenchyma involving basal ganglia
and deep white matter structures. New cystic-appearing lesion right cerebellar peduncle. Given the history,
suspect cryptococcal meningitis.
Hospital course:
The patient underwent a left lower lobe lobectomy for the spiculated pulmonary nodule shown on CT Imaging The pathology confirmed that the adenocarcinoma was completely resected within the tissue submitted. The patient had a surgical cure of his lung cancer.
Results of the lumbar puncture:

Organism Identified: Cryptococcal neoformans
The lumbar puncture did show evidence of yeast on the smear of the spinal fluid concerning for cryptococcus. All cultures of his
CSF revealed cryptococcus.
There was lymphocytic pleocytosis. A predominance of lymphocytes is not characteristic of an acute meningitis (neutrophils).
The protein was elevated and the glucose was low. An opening pressure is useful to determine the risk of increased intracranial pressure. It was a pressure of 10 (normal <20).
Hospital Course:
The Patient was started on IV Amphotericin B (Abelcet form) 400mg q24hr along with flucytosine 2,000
mg PO q6hr. He recovered well from the lung surgery, gained strength, and improved from his dizziness and confusion. His hallucinations gradually resolved.
Overview of Cryptococcal meningitis
Cryptococcal meningitis is caused by Cryptococcus neoformans, an encapsulated yeast that is found ubiquitously in the
environment. C. neoformans is considered to be an opportunistic fungus, as it typically does NOT lead to
infections in those with fully functioning immune systems. It gains entry into the host through the pulmonary routes. It can lead to primary lung disease but has a tropism for the brain and can cause cryptococcomas (as in the above patients) and cryptococcal meningitis. Infections of the skin and other organs and tissues can occur. Although infections may rarely be seen in persons who have no obvious immune-compromising condition, typically infections occur in patients with conditions such as HIV, organ transplants, corticosteroid use, impaired cell-mediated immunity, or other immune compromised states (2)
Cryptococcus often presents as pneumonia, however, it spread to the CNS leading to meningitis and often the yeast will accumulate forming cryptococcomas (1) .
Cryptococcus neoformans typically infects immunocompromised individuals, but another species Cryptococcus gattii (formerly
known as Cryptococcus neoformans gattii) has been shown to more often infect immunocompetent
individuals (1).
Cryptococcus gattii was formerly seen largely in Australia, however since 1999 emerged on
Vancouver Island and has spread to the Pacific Northwest of the United States. There have been numerous
case reports in patients without clear risk factors and competent immune systems who have been infected
with Cryptococcus gattii and subsequent cryptococcal meningitis (1) .
Malignancy and Cryptococcal meningitis: Cryptococcal meningitis is not seen as a common infection in
patients with risk factor being malignancy alone, however is seen in patients with malignancy who are
undergoing treatment, especially with steroids as part of their therapy as their immune system is
compromised during therapy (5). A retrospective review was performed in 2001, looking at 31 patients with
cancer (6 of whom had cryptococcal meningitis) who did not have known HIV infection. Overall, this
retrospective study revealed that patients with cancer as their only known risk factor showed to have a good
therapeutic outcome. Treatment of these patients varied with only 18% treatment failure and good success
with fluconazole as monotherapy alone (5).
Diagnosis: Fungal meningitis is typically more subacute compared to the acute nature of bacterial meningitis.
Signs and symptoms include: progressive headache or severe headache, signs of meningismus (photophobia,
nuchal rigidity, and headache), impaired cognitive function, confusion, coordination and gait disturbances,
behavioral/personality changes, and reduced visual acuity or visual disturbances. Patients commonly will have
nausea and vomiting, and fever.
Tests for diagnosis (3):
-CT/MRI revealing enhancement, parenchymal lesions and sometimes hydrocephalus.
-Fungal blood cultures may be positive or negative
-Serum cryptococcal antigen test
-CSF opening pressure: typically, elevated.
-CSF WBC: elevated (fungal meningitis typically reveals lymphocytic pleocytosis -20 to 500 cells/mL). May be normal in cases of HIV associated cryptococcal meningitis
-CSF protein: elevated
-CSF glucose: low
-CSF in India ink: positive
-CSF culture: may be positive OR negative
-CSF coccoidal IgG antibodies: positive
Treatment (1,2,3):
Treatment varies from patient to patient; however typical treatment recommendations are outlined
below. Treatment often begins with initial induction therapy (induction is a term that often is used in
cancer treatment which described the first series of therapeutic measures taken in treatment).
Induction consists of IV antifungals (e.g. Amphotericin B plus flucytosine/fluconazole) for about
2 weeks (3)
After induction is complete, consolidation therapy 3 is initiated. Consolidation is with
fluconazole orally once daily for 8 weeks. After consolidation, maintenance therapy is initiated. Patient can be started on low-dose
fluconazole for long-term therapy. The length of treatment depends on immune compromised
state, and it is not clearly defined how long patients should remain on therapy and without data
should be up to the discretion of the provider (3).
Back to the Case:
The patient described in this case received 19 days of IV Amphotericin B plus flucytosine. His most
prominent symptoms of headache, nausea/vomiting and mental clouding improved with the IV
therapy. He had a repeat lumbar puncture which did not grow organisms and had a decreased opening
pressure of 8cm. He was then transitioned to oral fluconazole planned for 6-12months, with potential
for lifelong suppression. It was felt that the brain lesions were likely cryptococcomas rather than metastases.




Leave a Reply