Flashback: Intern Year
As an intern, I attended to a woman who was having an acute ischemic stroke. This occurs when a thrombus (or clot) blocks the pathway of an artery that supplies oxygen to the brain. She came in with significant aphasia (an inability to talk), facial droop, and contralateral (other side) arm and leg weakness. I reviewed the MRI with the neurologist, and we discussed the indication for thrombolytics (tPA) used to break the clot. She had a significant size of penumbra (area of brain edema around the clot-involved blood vessel), and was considered on the borderline side for tPA. When the area is too large, the therapy could provoke a brain hemorrhage (bleed). I asked the neurologist about it. He reassured me that she would tolerate it. I observed him giving the therapy and was relieved that there were no complications. However, about 24 hours later she coded, and I feared the worst case scenario. A STAT CT scan of her brain determined that she had the dreaded consequence of a brain bleed. About 4 weeks later, after a long hospitalization and getting ready for transfer to rehabilitation case, now on a different inpatient rotation, I rushed to her bed when a code blue was called. Sadly, she did not make it out of the hospital after her stroke.
In my mind, I walked back her stay and recalled the day we first met while she was having her stroke: she had a worrisome look on her face and I reassured her that it was going to be OK. It became imprinted onto me that stroke support require stroke prevention and advocacy. Both of these are part of the mission of the NW Brain Network that we are developing (see below for more details).
Questions:
- If you knew that one day you would have a stroke and it would drastically change your life, if not lead to your death, how would that affect the way you address your life now.
- Is preventing a first stroke possible, or is a stroke out of our hands and just bad luck?
- What about preventing the next stroke?

Stroke: Addressing the Risk Factors
Worldwide each year, an estimated 15 million people wake up to a new reality: a stroke. According to the WHO, 5 million people will die from a stroke. Of the 10 million survivors, half are left permanently disabled. After a stroke, a person must set aside their previous goals and aspirations to begin the uphill journey toward optimizing function. It is a course that often requires several months of physical therapy and is met with slow gains and long plateaus.
In the United States, strokes rank as the fifth leading cause of death. Approximately 795,000 people will have a stroke; 610,000 of these being the first stroke. A sizeable amount (185,000 people) will have another stroke within 5 years. Stroke is not just a problem for those of advanced age. In 2009, 34% of people hospitalized for stroke were less than 65 years old (source CDC).
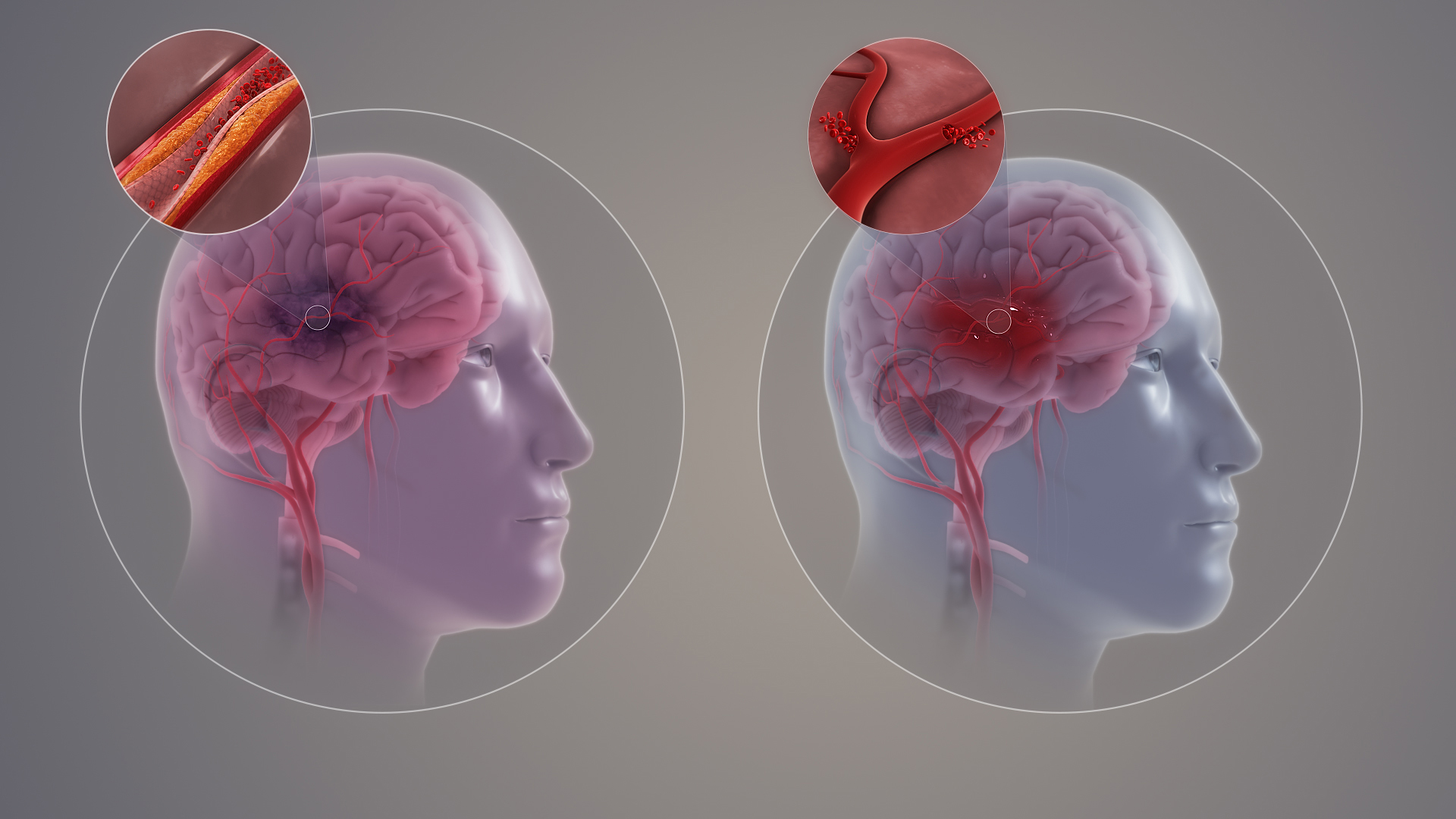
A stroke occurs when there is a disruption in the vascular supply of the brain, either after a brain bleed, a hemorrhagic stroke, or from a clot, an ischemic stroke. A person who develops a stroke often has multiple risk factors related to chronic metabolic disease, including high blood pressure, diabetes, coronary artery disease. The presence of these conditions is seen in as many as eighty percent of individuals presenting with stroke.
Aim of this post: With such high-stake consequences after a stroke, the greatest likelihood of a substantial reduction in disability is to prevent the first stroke from ever happening. Promoting optimal vascular health is an objective in reducing the risk of a stroke. The health of the cardiovascular system often mirrors the complete optimal health, so that vascular health entails overlaps lack of chronic disease, reduced infection risk, reduced likelihood of dementia. To address prevention, we need to discuss about how these diseases are inter-related.
Stroke: a Health Equity Issue
There is no coincidence that stroke mortality rates overlap with the highest obesity and diabetes prevalence. In the United States, the area of highest prevalence for these conditions is in the southeastern United States. The area of higher stroke mortality risk spans the poorest states.
If you are African American or Latino, you have a two-fold higher risk of stroke, and at a younger age, than someone not in these groups. Not only is stroke more common in these groups, it is more likely to be deadly. The stroke risk likely is due to concomitant conditions, such as obesity, high blood pressure, and diabetes. These disparities in stroke based on geographic and background point to a major health equity gap that requires attention in program and budgetary planning.


Adult obesity rates in the U.S. by state (2013) (pink to dark red) 20.2–24.0% 24.0–25.0% 25.0–26.8% 26.8–28.7% 28.7–30.4% 30.4–32.7% 32.7–34.0% 34.0–35.2%


Stroke: Addressing the Risk Factors
There are multiple exposures that contribute to an increase risk of a stroke. Suffice it to say, that the body has an inflammatory response as a result of environmental exposures and internal reactions. How do exposures become processed by our bodies? They gain access to our vascular system either through our respiratory tract, the air we breathe, or through our gastrointestinal tract, the food or drink we consume. The brain also processes stressors, perceived and real, and can even propagate inflammation through neurotransmitter and hormonal signals.
As you read through the list of risk factors, ask yourself if you have done everything that you can to protect your body from illness or dis-ease. Optimal health is a gift to yourself, and, when the systems are functioning in wellness, everything falls into synchrony. This is a promise that no medication can offer.

Smoking. The CDC estimates that the prevalence of smoking in the United States is approximately 20.8% of the population. There is a strong correlation to smoking and stroke risk, current smokers have a two- to fourfold higher risk of stroke compared to lifelong nonsmokers (or if individuals quit 10 years before). The amount of smoking increases the risks, what toxicologists call adose-response relationship. Smoking risks are not just limited to smokers but those that receive second-hand smoke (nearly two-fold increased risk). Data is emerging that areas with higher levels of air pollution in general also puts people at an increased risk of stroke.
Cigarette smoke inflames vessels and clogs arteries. The air and particulate contaminants of smoke are absorbed into the vascular system, unleashing inflammation that accelerates atherosclerosis. After smoking, multiple changes are found in the blood, including an elevated triglyceride level and LDL, a lower HDL, increased platelet aggregation, increased clotting factors (fibrinogen), increased inflammatory markers (cytokines) and increased oxidative stress. Suffice it to say, that changing the air that you breathe in by polluting it accelerates the changes seen with aging and puts a person at risk for all forms of vascular disease — including heart disease, stroke, aneurysm, and vascular impairment to the legs (claudication).
“The more you smoke, the more you stroke.”
Age. You can’t change your age, but you might be able to change the aging process in the body. Think of a healthy diet, exercise, and a healthy lifestyle being the ingredients to a healthy vascular system. Studies on supercentenarians show the relative lack of vascular disease, low incidence of Parkinsonism, diabetes, hypertension, and stroke, and an extended health span. This means that a person who makes it to this elite health category usually is fairly functional until the time of their death, with a short period of morbidity before. Vascular health is required for optimal health, and is the closest panacea to the fountain of youth.
High blood pressure (Hypertension). Hypertension is the most common risk factor of stroke. In patients presenting with stroke, 64% were found to have hypertension as a risk factor. In many patients, there are reversible risk factors for hypertension, including obesity, sleep apnea, excessive alcohol consumption, and certain medication intake (prednisone, nonsteroidal therapy, etc). If no clear conditions are determined, your doctor can embark on the work-up for secondary causes of hypertension.
Diabetes. Although diabetes results from endocrine pancreatic deficiency (Beta-islet cell dysfunction which produce insulin) and insulin resistance in adipose tissue, it is essentially a disease of the vascular system. As digested food is absorbed in the intestines through the portal bloodstream into the liver, a diet with excess glucose and certain types of fat induces hyperglycemia and various inflammatory reactions. In diabetes, lack of insulin activity causes glucose levels to remain too high in the bloodstream. Atherosclerosis occurs in an accelerated way, increasing the risk of stroke in a diabetes two-fold.
Atrial fibrillation. Atrial fibrillation (AF) affects 33 million worldwide. It can occur for different reasons but happens with the pacer signal in the atrial node or altered or disrupted. The atrial chambers and ventricles of the heart become asynchronous, leading to an increased risk of clot development. The clot is then projected toward brain circulation and gets lodged in one of the arteries producing a stroke.
AF likely represent 10-12% of all ischemic strokes. Although some people may not a decrease in exercise tolerance and a feeling of increased breathlessness, others may be asymptomatic. Other risk factors such as history of Congestive heart failure, High blood pressure, Age >75, presence of Diabetes, prior history of Stroke (CHADS2); additional factors such as the presence of vascular diseases (V), Age >65 (A) and gender female (Sc) can be used to determine the CHADS2-VASc score. The highest risk group has a 1 year event rate of 8.8 to 12.3%. Based on these scores, a doctor may prescribe aspirin alone or anticoagulation options, such as coumadin or a newer oral anticoagulant (NoAc).
Obesity. The CDC estimates that approximately 72% of the US population is either overweight or obese (40%). A person who is obese (BMI of greater than 30) ise 2 to 3 times more likely to have a stroke than someone who is in an ideal weight category (BMI <25). Obesity is associated with multiple chronic disease conditions, including hypertension, diabetes, and sleep apnea – all of which are risk factors for strokes.
High Hematocrit. An elevated hematocrit is an index of the red blood cell volume associated with increases in red blood cells, or polycythemia. This condition can be primary (meaning from overproduction of red blood cells from the marrow) or secondary. Common forms of secondary polycythemia include testosterone replacement, sleep apnea, and smoking. The first step in uncovering this condition is receiving a complete blood count by your physician.
Sleep apnea. Sleep is of utmost importance. The average person spends one-third of their life doing it. As we age or acquire health conditions such as obesity, opiate dependence, alcohol dependence and neuromuscular disorders, there is an increase in prevalence to a disruption in sleep patterns and sleep apnea. When a person has apneic (not breathing) or hypopneic (less breathing) during their sleep, the percent of oxygenated blood lessens and carbon dioxide rises. This increases pressures in the lung, signals the heart to beat harder, and consequently increases the blood pressure and heart rate. Consequently, sleep apnea can lead to hypertension and atrial fibrillation, both of which are associated with increasing the risk of stroke. The worse the apnea is, the more increased the stroke risk.
More than 12 million American adults are estimated to have some form of sleep apnea; as many as 80% are undiagnosed (and untreated). There is probably a good reason to screen for sleep apnea if your weight is above a BMI of 28, your age is greater than 50, and/or you have fatigue, high blood pressure, diabetes, chronic pain syndromes, “brain fog,” cognitive dysfunction, or hypotestosteronism (generic term for low measurement of serum testosterone – which can be from gonadal failure or secondary from sleep apnea). There is often a lot of resistance with getting a sleep study (polysomnogram), unless someone is truly having sleep disturbance, even though they may feel fatigue. Our judgement of our sleep performance is often imprecise.
Stroke patients should be screened for sleep apnea after the first episode, since sleep apnea is an independent risk factor. In the near future, I would like to see everyone have access to a home polysomnogram study when they are fifty, just like we “gift” patients with colonoscopies on that birthday. It is crucial to the understanding of the homeostasis of the body with a dynamic test such as a sleep study.
Carotid/Coronary artery disease.
As many as 8% of all ischemic strokes are attributable to carotid artery diseases, the presences of atherosclerosis in the main arteries to the brain. In someone who has presented with a stroke and is found to have severe carotid artery stenosis (greater than 70% blockage related to atherosclerosis), there is a reduction in recurrent strokes in those that had the stenosis addressed. The typical procedure is known as carotid endarterectomy, which my patients sometimes call “roto rooter” of the carotid artery.
Vascular disease in one part of the body is associated with vascular disease in other parts. The circulatory system extends to every space of the body that has living cells, and various inflammatory triggers follow the network. Just by having had a history of Myocardial Infarction (heart attack), there is a 44-fold increased risk of stroke within 30 days after an MI, and an increase risk of stroke in the year following. The long-term risk remains higher, at 1.6 times.
Alcohol intake or Stimulant drug use. Substances such as alcohol and stimulant drugs such as methamphetamine and cocaine raise the blood pressure and heart rate (in the case of methamphetamines). One meta-analysis (several studies analyzed), showed approximately a 20% increased risk in those that consumed alcohol heavily (relative risk of 1.2). Methamphetamine use can increase the risk of stroke. predominantly hemorrhagic, regardless of age. This is attributable to the drugs effects: high blood pressure, vascular inflammation (vasculitis), toxicity to vessels, and spasm of vessels (vasospasm).
Physical Inactivity. Vascular health is protective against stroke, and physical activity promotes vascular health. Various studies have demonstrated that greater activity was associated with a 25% to 64% lower risk of stroke incidence or mortality compared to the lowest active groups. Lack of physical activity may also be a poor prognosticator after a first stroke. Inactivity is hazardous to your health.
Hypertriglyceridemia. A lot of effort is spent in the clinic screening cholesterol levels to determine risk for heart disease. Clinicians often focus on “good” (HDL) and “bad” (LDL) cholesterol, without as much effort placed on the triglyceride value. Prospective studies did not show increased cholesterol intake was associated with an increased risk of stroke. The presence of elevated LDL and cholesterol levels also was not established to be a major risk factor for stroke. However, the triglyceride level stands out as an independent risk factor for stroke. The basis for this risk may be how it induces inflammation.

Stroke Risk: From years to days before
Over the course of years and stretching into decades, a relative degree of compensation, in the setting of being overweight or obese, shifts gradually toward a more decompensated state. A person may develop vague symptoms of feeling tired and weak, restless nights, or have leg swelling. There may also be more concerning diseases states, such as diabetes and elevated blood pressure.
Although these conditions are usually addressed as separate diseases, they represent a spectrum of illnesses seen when the body undergoes inflammatory changes that accelerate vascular aging. r many years. The body shows signs of changes from aging of the vascular system.
Studies that evaluate the extent of atherosclerosis, such as the coronary artery calcium score (CAC), show a strong correlation to calcium in arteries of the heart and stroke and heart attack risk. In one study, 95% of the individuals who had a stroke had a measurable calcium score; those with a score above 100 had a two to threefold higher risk of stroke or heart attack.

Magnetic Resonance Imaging has uncovered white matter lesions (consistent with demyelination – or deterioration) in the brains of individuals with chronic diseases without stroke. Likely, these changes are occurring from impaired oxygenation (ischemia). As a physician evaluating people with dementia, I often had MRIs come back with “microvascular ischemic white matter changes” or leukoariaosis; sometimes “compatible with normal changes of aging.” These changes were seen in patient’s with poor vascular health and I often determined them to have moderate to severe sleep apnea. I would not consider them “normal.” Consider these changes on MRI an indication for disease modification, such as optimizing weight (obesity and its association with high blood pressure), smoking cessation, and sleep apnea screening.
One study evaluated individuals for the accepted risk factors of stroke: including hypertension, diabetes, smoking, hypercholesterolemia and cardiac disease. An increase in risk factors was associated with an increase in white matter lesions on MRI; the greatest intensity was seen in those with arterial hypertension, hypercholesterolemia, and diabetes (Lechner et al, 1987).
Stroke: The Day

What is a Transient Ischemic Attack (TIA)?
A person presents to the hospital with a sudden change in neurologic status, but the symptoms subside over hours without any permanent changes. This is known as a TIA. A consensus definition of a TIA is a “transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia (decrease in blood supply), without acute infarction (death of tissue).
Consider a TIA the last warning prior to the permanent changes of a stroke. As many as 4% to 20% of patients who have had TIAs will progress to a stroke within 90 days; in one study, 5.1% of people with a TIA have a stroke within 48 hours. A TIA is a high predictor of a future stroke.
On the day of the stroke, a person may spend the morning on usual activities. If they are like most people, they may not have ever needed to see a doctor for an emergency. An estimated 60% of Americans don’t know they are at risk for a stroke. Maybe they were told that they had a “touch of sugar (diabetes)” or a “little bit of pressure.” Since these conditions manifest along a spectrum, they may have not regarded it as a significant risk for a stroke.
They may be among the 14%-25% of people (approximately 58,000 people in the US) who suffer a wake-up stroke. The most likely time of the day for a heart attack and stroke is in the morning, at 6:30 AM. This may be related to the effects of sleep apnea, which results in dips of oxygen levels, fast heart rates, and increased blood pressure. They may even present on the day of the stroke with atrial fibrillation.
Acute warning signs and symptoms

Facial droop
Arm drift
Speech problems
Time to call 9-1-1

Stroke Day 1 and Beyond
The clock starts ticking the moment a person has signs of stroke. It is almost as if a reset has been made, drastically modifying a person’s reality. When a person is admitted to the hospital for acute care, the average stay is between four (ischemic) and seven (hemorrhagic) days. There they receive multiple diagnostic tests to try to confirm the reason of the stroke and possibly to receive an intervention, if they are candidates. Next, he/she is transferred to a rehabilitation hospital, where they can undergo intensive physical therapy. Studies show that the most significant period of recovery is within the first three months after a stroke, where most 48 to 91% of the recovery occurred. Nevertheless, efforts toward preventing a second stroke with intensive rehabilitation and health improvement would ensure ongoing neurological improvements even after several months or longer. Hebbs theory, “if it fires, it wires,” applies to developing new neural connections to compensate or bolster damaged connections following a stroke.
Summary
The article attempts to place an emphasis on the risk factors that contribute to a stroke, which can sometimes occur many years before. I shared with you a dramatic presentation of someone with an ischemic stroke which became hemorrhagic following thrombolytics. She was among the one-third people presenting with stroke that do not survive.
Since a stroke has such a significant impact on a person and the family support, an effort toward primary prevention may protect someone from the drastic life consequences of a stroke. If you have any of the above risk factors, make it a priority to address these Now. Refer to Your Health Forum in the Overcoming Obesity and Finding Wellness sections, which can further guide you along this path. Please consult with your doctor for specific concerns related to your health.
Resources:
1. References are embedded in the writing
2. What are your chances of having a stroke:
Stroke Risk Calculator
3. Information of the Northwest Brain Network, including events, articles, community blogs, and online conferences
Post-Stroke Neuroplasticity




Leave a Reply