History of Presenting Illness:
55 year old man with insulin-requiring diabetes mellitus and diabetic polyneuropathy with right foot ulcer presents to the Emergency Department with pain in the suprapubic area radiating into the rectum and shaking chills.
- He went in a river to fish 4 weeks ago and developed a blister around his diabetic ulcer; it swelled up but there was no obvious purulence.
- About 4 weeks ago, he developed fever and chills and thought he was coming down with a cold; symptoms gradually subsided after 3 days.
- 4 days prior to presentation, he noted onset of fatigue.
- The next day, he noticed the onset of fever and chills.
- The day of admission, he developed fullness in the bladder and deep pelvis. He decided to go in, because he thought he might need antibiotics.
Review of Systems: Gen: +fevers, chills; GI: no nausea, vomiting or diarrhea Lungs; no cough or shortness of breath, 12 point other than above was negative
Past Medical History:
- Diabetes mellitus with polyneuropathy – prior surgery on left foot 2 years ago. Last A1c was 10.0 one month ago
- Hypertension
- Hyperlipidemia
- Recent admission for ulcer debridement in setting of acute cellulitis (right foot) – 2 months ago; Group B Strep grew on culture. He had prior exposure to keflex
- Rosacea, papulopustular – he mentions that 3 days before he became ill, he saw a pustule on his lid and expressed it. He uses clindagel and topical hydrocortisone
Social: No smoking or alcohol; he quit smoking after recent hospital visit
Fam HX: noncontributory
Meds:
- Lantus insulin 60 units daily
- Novolog 15 units pre meal with sliding scale adjustment
- Lisinopril 20mg daily
- Atorvastatin 20mg qhs
All: sulfa
Physical Examination
VS: T 102.3, HR 115, BP 100/50, Resp 16 bpm, Pulse ox 98% room air
Gen: Appears acutely ill, moderate distress from suprapubic and posterior pain
HEENT: No thrush or ulcers; Lymph: no axillary, cervical or supraclavicular LAD. Neck: Supple, nonrigid, trachea midline
Chest: Hs1s2, tachycardia, no murmur, click, rubs or gallops; Lungs: no wheezes, rales or rhonchi
Abd: suprapubic tenderness suggested, Rectal: Declined.
Extremities: Right foot: dry, calloused diabetic foot ulcer, slightly malodorous, no evidence of expressible fluctuance or erythema on examination.
Neuro: Cranial nerves 2-12 intact, non-focal
Laboratory and Radiographic Investigation:
- Wbc: 25,000, Neutrophils 85%, Lymphoctyes 10%
- H/H: 12/36, Platelet 95,000
- Chemistry: BUN 26, Creatinine 1.2
- LFT: AST 200, ALT 150, Alk phos 159

Discussion Questions:
Question 1: What does this CT scan show?
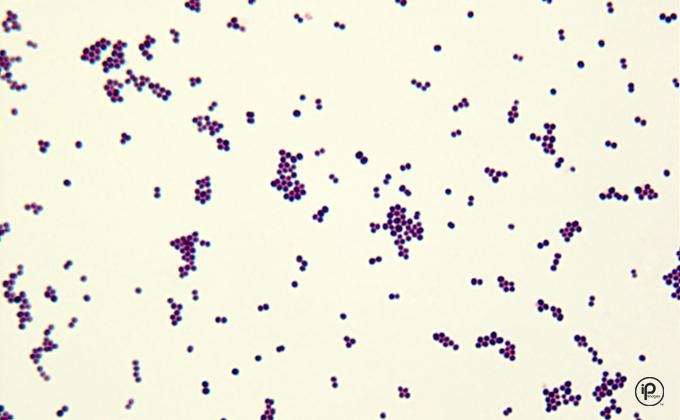
Question 2: The patient was found to have 6/6 positive blood cultures for an organism that was also found in his urine culture (spoiler below). Given his particular presentation, which microorganism is likely to be the cause?
Question 3: The patient is hospitalized for this presentation. Which antibiotic(s) would be appropriate to start with?
You can find the answers here.





Leave a Reply