Question 1: What is being shown on CT scan?
The CXR is showing what appears to be air-fluid levels in the right pleural area on the radiograph and is confirmed on the CT scan with fluid and air within the right pleural space. The lung parenchyma of the left base appears to show significant bullous changes of COPD. Given these bullous changes he may have developed a pneumothorax at the time of the acute worsening. Such findings are consistent with a bronchopleural fistula.
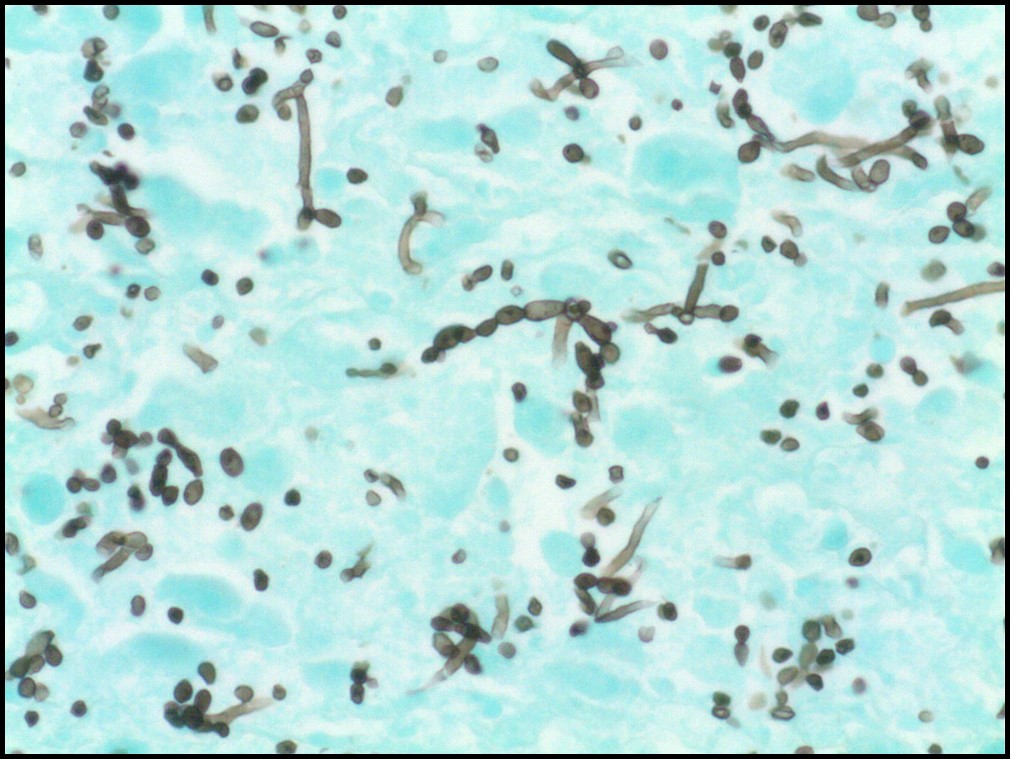
Question 2: What is the name of the specialized stain shown above? Why is it used?
The specialized stain is known as a GMS stain (Grocott’s methenamine silver). It is useful for staining the carbohydrate-laden cell wall of fungal organisms, such as Candida sp, Pneumocystis jiroveci, Coccidiodes sp and Cryptococcus sp.. The H & E stain showed significant neutrophils present in the tissue consistent with a lung abscess.
Question 3: What is shown using this specialized stain?
The organisms that are shown have evidence of pseudohyphae and is consistent with the typical microscopic appearance of Candida species.
Question 4: What do you suspect was the diagnosis and likely risk factors? Hint: Risk factors are from history, hospital course and discovered (at least 3).
The diagnosis is Candidal lung abscess, Right lower lobe with bronchopleural fistula and empyema.
Likely, this patient with bullous COPD originally had a viral pneumonitis. He had acute respiratory distress and was treated with broad spectrum antibiotics and a prolonged course of steroids (IV solumedrol). Steroids and antibiotics promote the growth of Candida species in the oropharynx. After five days, he had a bronchoscopy procedure, which may have pushed the Candida into the deeper airways. On account of ongoing inflammation and likely compromised tissue associated with ventilator pressures, he developed a pneumothorax at some point during the infection.
Thank you for reading this week’s ID case report challenge!




Leave a Reply